Curative surgical treatment
![]() When
you see this type of reconstruction take place through the magic
of biology the reply is clearly yes. This is why the use of natural
coral to fill a bone void, both contents and container, seems to be so
valuable.
When
you see this type of reconstruction take place through the magic
of biology the reply is clearly yes. This is why the use of natural
coral to fill a bone void, both contents and container, seems to be so
valuable.
![]() Let's
go back over the various techniques for reconstructing this unfortunate
broken bone. Everyone agrees to the need for this repair. The bone must
have its continuity restored so that the patient can walk again, but opinions
diverge on how to rebuild the bone, with respect to technical resources
and which is just as important on what should be done
when there are several pieces.
Let's
go back over the various techniques for reconstructing this unfortunate
broken bone. Everyone agrees to the need for this repair. The bone must
have its continuity restored so that the patient can walk again, but opinions
diverge on how to rebuild the bone, with respect to technical resources
and which is just as important on what should be done
when there are several pieces.
![]() In
brief, bone continuity must be restored but the question is, how, which
means, with what?
In
brief, bone continuity must be restored but the question is, how, which
means, with what?
Which technique should we start with?
![]() There
are two schools of thought, one supporting the idea of rigid fixation
and the other that of mobile fixation. One uses metal rods inserted into
the bone, roughly in the shape of a Greek
There
are two schools of thought, one supporting the idea of rigid fixation
and the other that of mobile fixation. One uses metal rods inserted into
the bone, roughly in the shape of a Greek ![]() .
The other uses one screw screwed into the head of the femur and a plate
screwed outside the bone. They are linked by a hollow tube which makes
an anatomical angle with the plate to which it is joined. The screw and
tube-plate can slide in and out of each other. In fact, only the tube-plate
slides along the length of the screw which is fixed into the head of the
femur and cannot, therefore, be moved.
.
The other uses one screw screwed into the head of the femur and a plate
screwed outside the bone. They are linked by a hollow tube which makes
an anatomical angle with the plate to which it is joined. The screw and
tube-plate can slide in and out of each other. In fact, only the tube-plate
slides along the length of the screw which is fixed into the head of the
femur and cannot, therefore, be moved.
![]() Without
going into the arguments, neither of the two solutions suggested was concerned
with the cause, i.e. the bone loss, which affected both the container
(the walls) and the content (inside) of the bone. Neither of these methods
regenerated bone in the bone. Neither of them took the bone into consideration.
This is a simple fact.
Without
going into the arguments, neither of the two solutions suggested was concerned
with the cause, i.e. the bone loss, which affected both the container
(the walls) and the content (inside) of the bone. Neither of these methods
regenerated bone in the bone. Neither of them took the bone into consideration.
This is a simple fact.
![]() Concerning
the attitude of traumatologists with respect to various fractures, the
same indifference is noted. Both techniques agreed that the two largest
fragments of broken bone should be reunited, either by a nail (the Gamma
Concerning
the attitude of traumatologists with respect to various fractures, the
same indifference is noted. Both techniques agreed that the two largest
fragments of broken bone should be reunited, either by a nail (the Gamma
![]() nail) or by the
screw-plate. Here is an example of a simple fracture with the two biggest
fragments.
nail) or by the
screw-plate. Here is an example of a simple fracture with the two biggest
fragments.
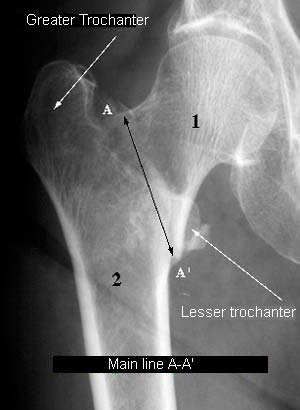
![]() A
fracture line (A-A') can be seen, separating a large upper fragment (1)
and a large lower fragment (2). This is the main fracture line. These
are the two basic fragments. They are always found in a femoral neck fracture.
This is the traumatologists' only concern.
A
fracture line (A-A') can be seen, separating a large upper fragment (1)
and a large lower fragment (2). This is the main fracture line. These
are the two basic fragments. They are always found in a femoral neck fracture.
This is the traumatologists' only concern.
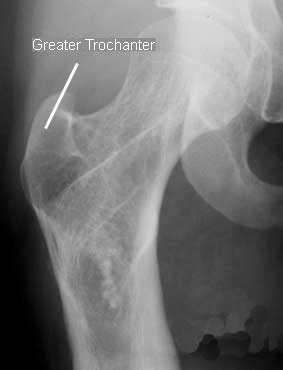
![]() Sometimes
the fracture is more complex and several other fragments may be detached
from these two main pieces. The secondary lines detach them. These lines
are usually neglected.
Sometimes
the fracture is more complex and several other fragments may be detached
from these two main pieces. The secondary lines detach them. These lines
are usually neglected.
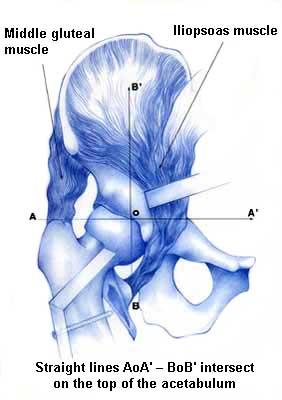
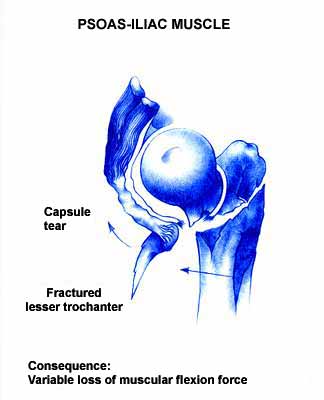
![]() Two
fragments are particularly important, however, because they are used when
standing, walking and going up and down stairs. They play an essential
part in the function of this weight-bearing joint. These are fragments
(apophyses) which are essential to hip physiology, i.e. to correct function
of this joint. They are detached by secondary lines. They are the greater
and smaller trochanter attached to fragment 2.
Two
fragments are particularly important, however, because they are used when
standing, walking and going up and down stairs. They play an essential
part in the function of this weight-bearing joint. These are fragments
(apophyses) which are essential to hip physiology, i.e. to correct function
of this joint. They are detached by secondary lines. They are the greater
and smaller trochanter attached to fragment 2.
![]()
Where are the greater and lesser trochanter located? What do they do ?
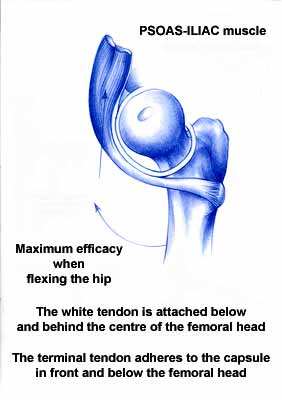
![]() Here
is an adult femur seen from the front and from the side. The two most
frequently broken fragments, which are detached under muscular influence,
form a sort of bony "protrusion" on each side of the two main
fragments.
Here
is an adult femur seen from the front and from the side. The two most
frequently broken fragments, which are detached under muscular influence,
form a sort of bony "protrusion" on each side of the two main
fragments.
 Front view |
 Side view |
![]()
|
||
|
||
|
||
|

![]() Neither
of the two classic techniques involves fixing these two "secondary"
fragments. Perhaps this is one of the reasons why there is a 75% record
of functional sequelae. These sequelae include more or less pronounced
limping and difficulty in going up or down stairs.
Neither
of the two classic techniques involves fixing these two "secondary"
fragments. Perhaps this is one of the reasons why there is a 75% record
of functional sequelae. These sequelae include more or less pronounced
limping and difficulty in going up or down stairs.
![]() In
any case, although a femoral neck fracture no longer has a "bad reputation",
it can lead to extremely disabling sequelae. The high rate of these sequelae
(75%) can only be lowered if the bone's continuity is fully restored to
bring it as close as possible to the anatomy.
In
any case, although a femoral neck fracture no longer has a "bad reputation",
it can lead to extremely disabling sequelae. The high rate of these sequelae
(75%) can only be lowered if the bone's continuity is fully restored to
bring it as close as possible to the anatomy.
Further information on current classical treatment of
femoral neck fractures
is available on theSpringer-Verlag
(EJOST) and Masson
(RCO) websites.
![]()
| Next page |