Revelation of bone loss
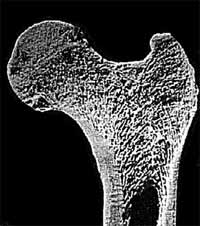
What does healthy bone and osteoporotic bone look like?
|
|
 |
|
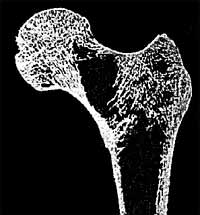 |
![]()
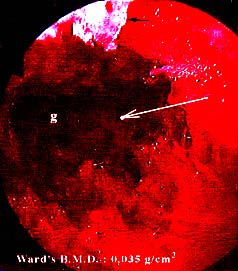
Can bone loss be detected on standard X-rays?
![]() When
there is major bone loss, this can be seen in the form of a "bony
void". It can be located via the missing trabeculae which form an
arch-shape in healthy bone.
When
there is major bone loss, this can be seen in the form of a "bony
void". It can be located via the missing trabeculae which form an
arch-shape in healthy bone.
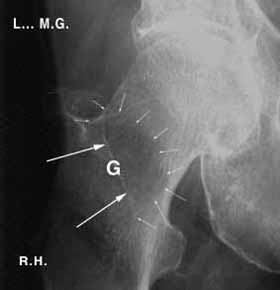 Void detected in a non-fractured bone |
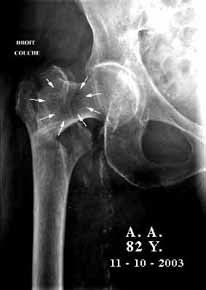 Void detected in a fractured bone |
| The "hole" in the bone is shown by the white arrows in both cases | |
![]()
Is it possible to "materialise", to "see" directly inside a bone?
![]() When
it is a healthy adult bone, it is impossible to see inside it because
of its compactness. A hole can be drilled and a camera inserted to record
"something", but this "something" would not give a
picture of what really goes on inside the bone because the manipulation
itself creates iatrogenic lesions – which means lesions created
by external intervention – in this case the drilling process and
camera insertion. This examination would lose all its scientific value.
When
it is a healthy adult bone, it is impossible to see inside it because
of its compactness. A hole can be drilled and a camera inserted to record
"something", but this "something" would not give a
picture of what really goes on inside the bone because the manipulation
itself creates iatrogenic lesions – which means lesions created
by external intervention – in this case the drilling process and
camera insertion. This examination would lose all its scientific value.
On the other hand, if there are already holes, notably due to osteoporotic
disease, a camera can be inserted to examine the walls and explore the
various cavities, their site and size, and describe what can be seen.
![]() This
is a bone endoscopy. This examination is equivalent to an arthroscopy
in which the camera penetrates a joint cavity, or a coelioscopy in which
the camera penetrates the abdominal cavity.
This
is a bone endoscopy. This examination is equivalent to an arthroscopy
in which the camera penetrates a joint cavity, or a coelioscopy in which
the camera penetrates the abdominal cavity.
![]()
One question: Isn't it possible for the camera to create lesions?
![]() The
camera only records what it is in front of it, during its progress into
deeper regions. The neck of a femur is four or five centimetres long.
When a solid obstacle is present, the operator does not go past it. If
he can get round it he does so.
The
camera only records what it is in front of it, during its progress into
deeper regions. The neck of a femur is four or five centimetres long.
When a solid obstacle is present, the operator does not go past it. If
he can get round it he does so.
Otherwise he points the lens in another direction and continues recording
what can be seen in front of it.
![]()
| Next Page |